Following his presentation at the 2026 CDISC EU Interchange in Milan, Ricky Lakhani shares his key takeaways on one of the most pressing challenges in clinical operations: harmonising Trial Master File (TMF) ecosystems through interoperability and standardised data flow. In this blog, he explores why connected systems and industry standards are essential to improving efficiency, compliance, and oversight across clinical trials.
I recently had the opportunity to speak at the 2026 CDISC EU Interchange, where I shared my thoughts on a continued challenge in clinical operations: harmonising Trial Master File (TMF) ecosystems through interoperability and standardised data flow. For those who couldn’t attend, or for anyone looking for a quick summary of my session, I wanted to distil the core message into this post.
For too long, the eTMF has been treated as a passive, retrospective digital filing cabinet - a place where documents simply go to rest once the real work is completed. However, as our clinical architectures become more complex, this siloed approach is no longer sustainable. We need to move beyond the static repository and transform the TMF into a living, breathing command centre for trial health.
The Evolution from Retrospective to Agentic
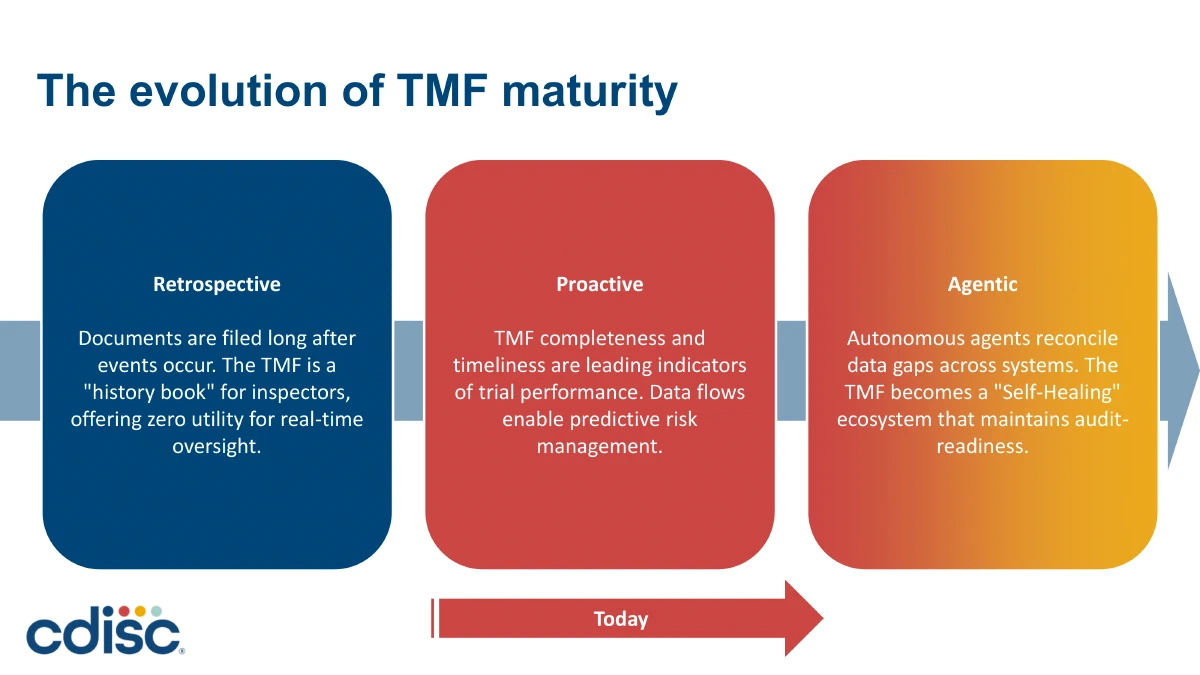
During my presentation, I outlined the evolution of TMF maturity. We are moving away from the “retrospective” era, where documents were filed long after events occurred and the TMF merely served as a history book for inspectors. Currently, many organisations sit in the “proactive” phase, using system integrations to spot compliance bottlenecks in real-time.
However, the future, and in many ways, the present, is the “Agentic” TMF. This means moving from systems that just store data to intelligent solutions that actively assist us. By leveraging Agentic AI (Artificial Intelligence), the system behaves like an autonomous digital assistant rather than merely following rigid rules. Practical applications include autonomous reconciliation (such as cross-checking CTMS visit reports against eTMF documents), self-healing metadata correcting naming convention errors, and intelligent site triage proactively managing missing certifications.
Navigating AI and Regulatory Expectations
Naturally, introducing AI into clinical systems prompts regulatory questions. The good news is that agencies like the Food and Drug Administration (FDA) and the European Medicines Agency (EMA) are open to this innovation, provided we implement strict guardrails.
If we use AI to auto-classify documents, regulators require a “Human-in-the-Loop” approach, ensuring that high-risk decisions and final verifications remain under human oversight. They also demand clear data provenance and explainability; we must be able to trace exactly when AI tagged a document, who verified it, and the rationale behind the classification. Black-box models simply won’t suffice. Ultimately, AI is here to handle routine checks so our teams can focus on value-added quality control.
Bridging the Systems Divide
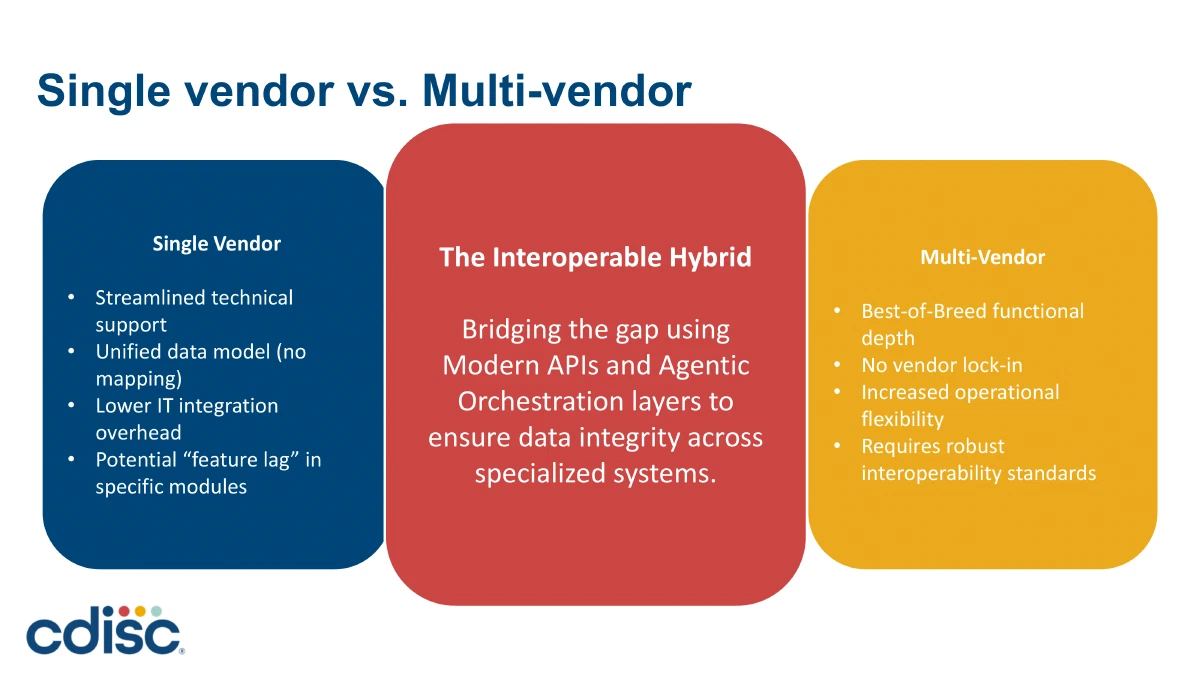
To enable this intelligent future, we must address the fundamental plumbing of our trials. Traditionally, clinical systems like the Electronic Data Capture (EDC), Clinical Trial Management System (CTMS), and Regulatory Information Management (RIM) have lived in isolation, resulting in systemic gaps and duplicate entry workflows.
Organisations face a choice between a single-vendor model (which streamlines support but may result in feature lag in certain modules) and a multi-vendor, best-of-breed approach. Historically, the multi-vendor approach brought a high integration burden, but modern web APIs, the continued evolution and adoption of data standards and agentic orchestration layers are bridging these gaps, allowing us to maintain functional depth without sacrificing data integrity.
Re-engineering the Human Element
Implementing interoperable technology is only half the battle; true change requires the re-engineering of our business processes. As we automate data flows, we need to shift our personnel away from being mere “document filers”. Instead, we must empower them to become data managers and AI orchestrators who manage data feeds and handle exception management. Furthermore, clinical operations, regulatory affairs, and data management must take cross-functional ownership of their data inputs rather than viewing the TMF as someone else’s problem.
A Clear Call to Action
When we get this right, the friction of study transitions, like CRO handovers or final close-outs, is significantly reduced. By finding documentation gaps during the active trial rather than at the end, study close-out becomes a verification exercise rather than a forensic search.
I closed my session with a practical roadmap and a threefold call to action for industry leaders:
- Audit your data leaks: Identify where your teams are still manually copying and pasting information between systems.
- Demand open standards: Protect your operational flexibility by insisting on true API compliance and standardisation from your technology and CRO vendors.
- Invest in change management: Improve AI literacy within your teams to prepare them for the data systems of tomorrow.
The eTMF is an active reflection of your trial’s integrity. Achieving true interoperability is not just an IT project; it is a strategic clinical imperative. I hope this summary provides a useful perspective on how we can build TMF ecosystems that actively breathe with our clinical trials.